Identifying the barriers to change
A long time coming
The costs of not reforming the UK’s care system are very high. NHS England has written extensively about the need for integration in the Five Year Forward View31, and The King’s Fund recently produced a very comprehensive paper on the topic32.
However, this is not a new desire for change. Consider this 1961 address to the National Association of Mental Health’s annual conference:
“…a hospital plan makes no sense unless the medical profession outside the hospital service will be able progressively to accept responsibility for more and more of that care of patients which today is given inside the hospitals. It makes no sense therefore unless the medical profession outside the hospital service can be supported in this task by a whole new development of the local authority services for the old, for the sick and for the mentally ill and mentally subnormal.”33
So why does the UK care system prove so resistant to change? What are the barriers?
Supply side inertia
The NHS is a state-controlled, supply-side monopoly. Clinicians deliver excellent care on the ground but are often confounded by the workings of the system, and especially by the constant reorganisations and initiatives – pilots, pioneers, vanguards – that supply- side monopolies of any sort too often mistake for change. Demand-side, needs-based, mechanisms are lacking in the system.
Who’s in charge?
There is a paradox that – despite the accountability and responsibility that secretaries of state, ministers, senior civil servants and senior NHS managers feel – lines of authority are tangled and lack cohesion. The picture is often so muddled that at times it can seem that no-one is in charge34.
The many dysfunctional dynamics within the system make the task of management an exceedingly difficult one. The strain is compounded by a sometimes rancorous attitude towards management which is often equated with bureaucracy or unproductive overhead. This is not an environment conducive to implementing transformational change35.
An under-supported workforce
The UK’s clinicians and carers are amongst the best and most dutiful in the world. However, they are often not given the right skills, are severely under-resourced, and in many parts of the system they are underpaid. For example, despite the government policy of moving people with mental illness back into the community, primary care physicians, nurses and carers are insufficiently trained in delivering mental health therapies. Similarly, the UK takes far longer to diagnose dementia than other major European countries.36
There is a shocking national shortage of nurses. In 2013, The Royal College of Nursing reported a shortage of 20,000 nurses and a 15 per cent reduction in the number of student nurses being trained, combined with an ageing workforce37. This issue continues to be dispiritingly unaddressed by government.
Meanwhile the drastic cuts in social care mean that, as of December 2012, more than 70 per cent of care workers were paid just £6.76 an hour38. This is only a fraction over the current minimum wage of £6.50, and considerably less than the pay for stacking shelves at Tesco. Poor wages are leading to high staff turnover and lack of care continuity.
Long-term care expenditure projected to increase sharply
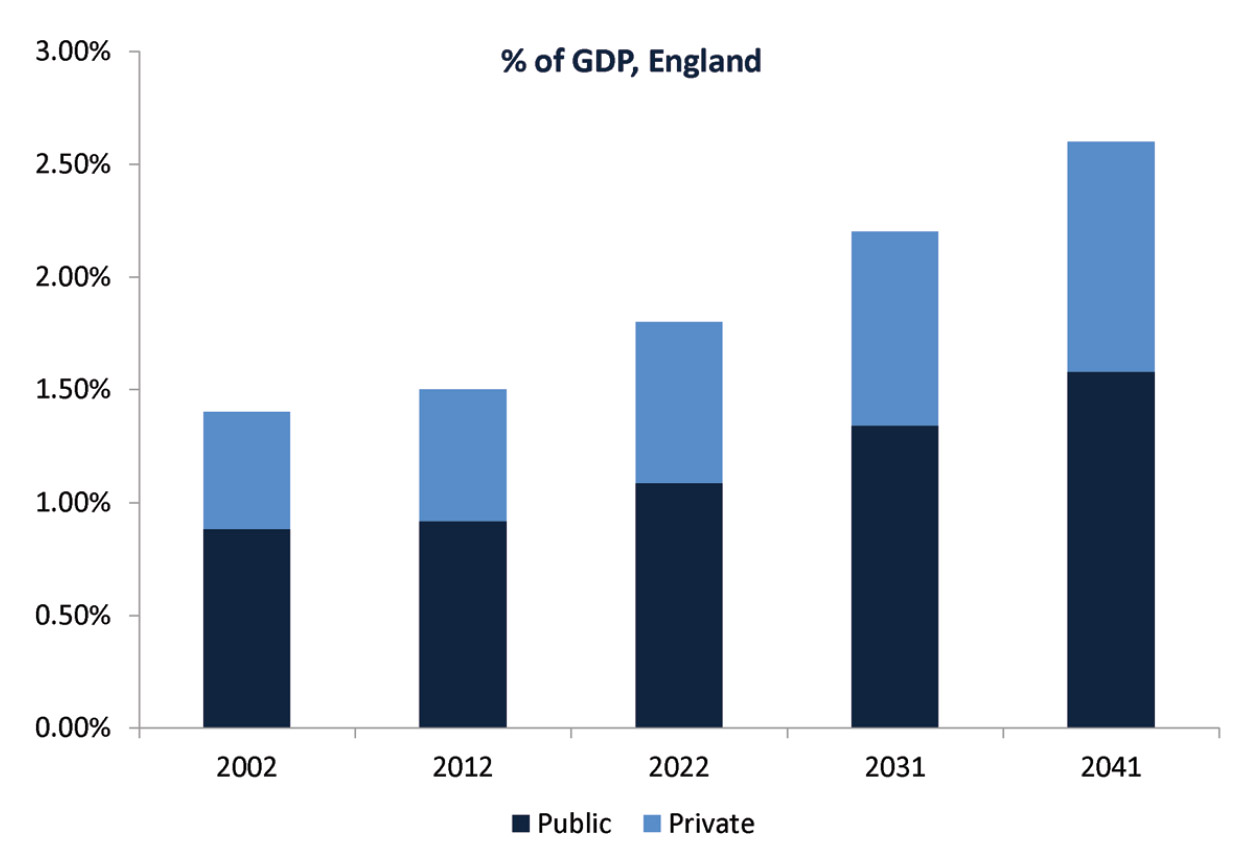

Wittenberg, R. et al (2006) Future Demand for Long-Term Care, 2002 to 2041: projections of demand for long-term care for older people in England tinyurl.com/careexpenditure
The problems of regulation
Regulation and inspection is fragmented and confusing. It is a patchwork of overlapping and often inconsistent regimes that include the Care Quality Commission, local authority inspectors and commissioners, Monitor, NHS England, and the Health and Safety Inspectorate. While the CQC, in particular, has made significant advances in the quality of its operations in recent times, the overall regulatory system is sometimes a distraction from real improvement in outcomes rather than supportive of them.
Constrained funding
We are not spending enough on health and social care. That the system is largely tax funded means spending per capita across the whole system will, due to the stringencies of austerity, fall over the coming years. Demand for healthcare is not going to fall. Social care funding has been at crisis levels for some time now. This too is set against a need that is rising rapidly.
A higher percentage of UK health spending is publicly funded compared to most other countries, and all of the public funding is drawn from the general taxation pot, unlike the more upwardly malleable social insurance system. This severely constrained funding means that the focus often has to be on carrying on, rather than on making the sort of fundamental changes that are needed.
The distraction of politics
Politicians play a major part in the negative processes of launching reorganisations, tinkering with day-to-day operations, overloading the capacity of the system with policy rather than action, and pioneering eye-catching initiatives.
Damage is also done by using the care system as a political football to score points in an attempt to garner votes. The real differences between informed politicians is actually quite small, but the temptation to mould a distinctive political portrait means that concerted action is grievously disrupted.