Our recommendations for change
Making the mechanisms work
As the previous section outlined, there are key mechanisms which can drive momentum for change. For these to be introduced, however, contextual changes will first be needed. These will address the longstanding barriers to wider change.
Put managers in charge, and support them
It is a paradox that we need less centralised, especially politicised, intervention into the care system, yet one of the first things we are recommending is centralised intervention. This is a matter of timing. The system is currently mired in a particularly messy marshland of fragmented, overlapping and discordant organisations and jurisdictions.
The inertia is so inveterate and long-standing that clear and determined leadership is required to launch the market mechanisms that we have outlined, and to drive the twin engines of ICO and AHSC. This leadership needs to come from the very top, through consolidation of health and social care at ministerial level, and then be invested in the CEO of the NHS (adding the social care responsibility). It needs to be complemented by decentralised leadership in local health economies, and full integration of health and social care budgets and teams.
Managers deserve and require full-blooded support in the change process, and they need an explicit plan to which they can orientate themselves and their organisations.
Their leadership and managerial skills should be actively enhanced. As Jenny Priest has pointed out: “It has been established that effective leadership is required to facilitate integrated care. This is clearly felt by doctors: when asked to identify the barriers to achieving integration through joined-up care pathways, over half of doctors responding to our survey felt that a lack of managerial leadership was a key barrier. Almost 44 per cent identified lack of clinical leadership as a barrier.”40
Boost the workforce, in number and skill
Workforce skills and numbers need to be increased. In the world of the ICO and AHSC, it is clear that clinicians need to be streamed depending on where they are going to deliver care. There will be more clinical specialists within hospitals, and more “extensivists” in a newly configured integrated system that breaks down the secondary/primary/social care distinctions.
GPs will need to further embody the extensivist concept, such that they can lead multidisciplinary teams in practices. These teams will care for complex patients and support a shift of care out of the acute hospital sector into the community – in nursing homes or in people’s own homes. Clearly the nursing workforce needs to increase.
Nursing homes should play a more important part in this process: entry level carers should have a nationally recognised qualification that lies between senior care assistant and state registered nurse.
This elevation of the skill level of the 500,000 care home workers in the country will require improved funding so that the United Kingdom breaks out of the vicious spiral of low pay, high turnover, limited clinical training, and compromised care.
Rationalise regulation
Rationalisation of the regulatory framework is urgent. Monitor and the regulatory functions of the TDA and NHS England should be closed down, and their activities should be integrated into a single regulator, the CQC, which itself integrated the regulation of healthcare and social care in 2009.
Find more money
Many of the recommendations in this pamphlet will mean that money is spent more efficiently and effectively – such as the reduced inappropriate use of expensive hospital beds for frail older people.
However, more money will also be needed. The UK is not spending enough on health and social care. The fact that the system is largely tax-funded will mean that spending per capita across the whole system will, due to the stringencies of austerity, fall over the coming years. Social care funding has been at crisis levels for some time now.
The proportion of gross domestic product (GDP) spent on health and social care should rise at least to the average levels across the more advanced parts of Europe (in 2012, the UK spent just over 9 per cent of GDP on its health service, compared to almost 12 per cent in France and the Netherlands).41
It is quite appropriate that, as need and affluence increase, society will wish to spend more on health and social care. There is also a strong case for increased spending to maintain the UK’s global lead in biomedical science, which earns the country significant amounts of foreign earnings.
The constraints to an expanding share of GDP being spent on health and social care is the fact that the majority of funding is derived from taxes and allocated by government.
Funding arrangements need to balance the solemn need to protect the most vulnerable in our society with the rising cost of the service. In the first place, this cost needs to be slowed by preventing flippant use of the system.
For example, many people would support a charge on drunken and abusive people attending A&E – at weekends it is estimated that 70 per cent of attendances between midnight and 5am42 are cases of drunkenness.
The austerity constraint to increased funding needs to be relaxed by placing more of the burden on those people more able to pay. In particular, the distinction between means-tested social care and a free at the point of care NHS needs to be eradicated. It will mean the wealthier people paying more (“top-ups”) for healthcare, and more money flowing into social care. This flow is a vital part of making the integration of health and social care work.
Finally, the debate needs to be launched on the advantages and disadvantages of a social insurance system. This is a highly emotive topic, and often triggers fears of a hidden agenda that will obstruct accessibility and compromise affordability.
A social insurance system is a more appropriate funding mechanism than the unedifying sight of the NHS chipping away at a limited slab of anonymous taxes. It shares risk based on the most needy, it is something to invest in, and it allows for the targeted financing of integrated care and therefore outcome priorities.
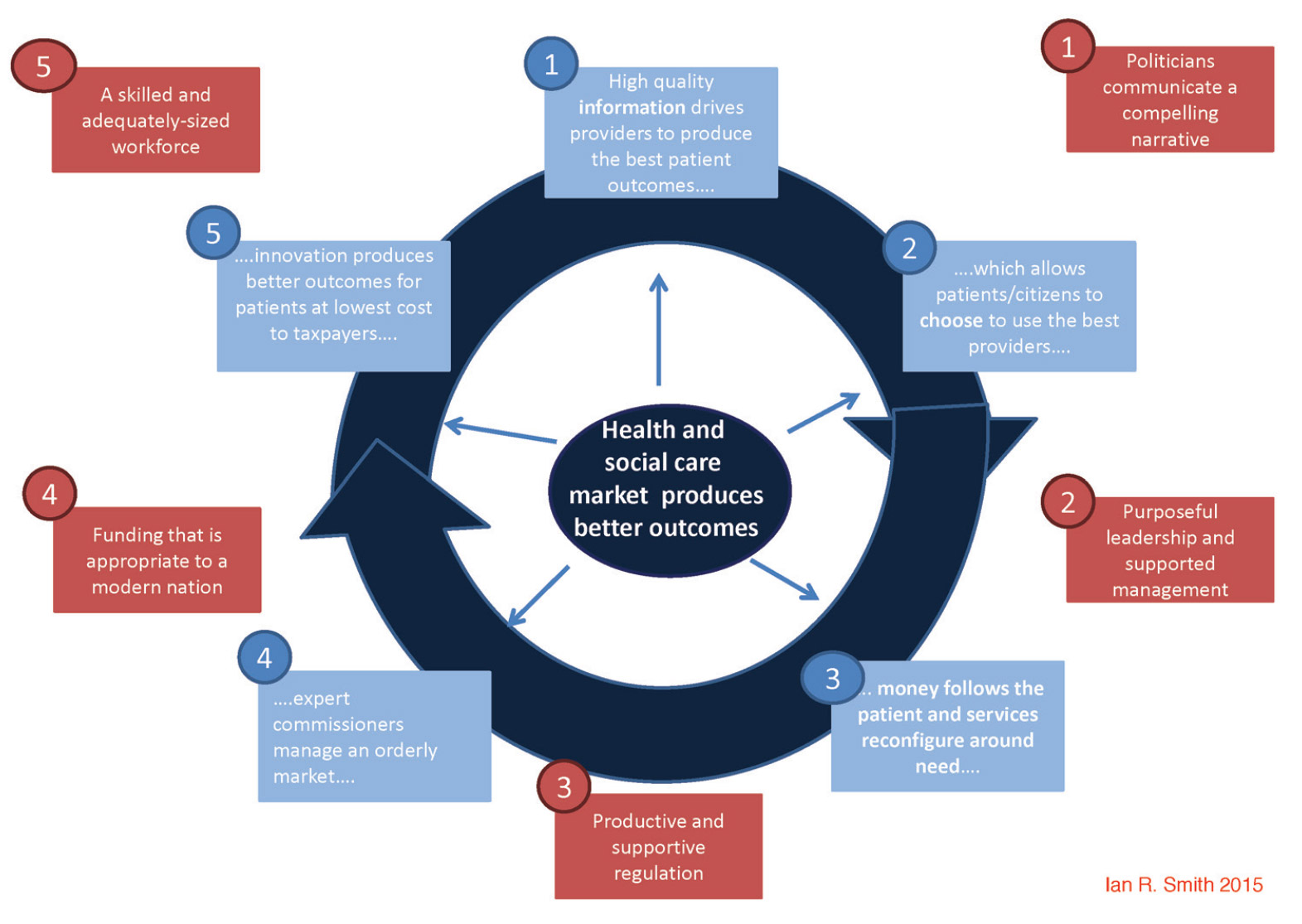
The virtuous circle driving integrated care, clinical excellence and scientific progress
A productive role for politicians
Politicians have an important role to play in the UK’s care system, but it is not the role they have traditionally played. The answer is to get the politicians out of the way of management and ban their often chaotic interventions. We need to say to our politicians what Dwight D Eisenhower is said to have commanded his meddling secretary of state, John Foster Dulles:
“Foster, don’t just do something; stand there”43.
The appeal should go out to the public that says demand more from your politicians, demand that they do what we pay them to do: to lead the country to a place that better serves its citizens. Some 73 per cent of respondents in a recent Ipsos MORI survey believed political parties’ policies on the NHS are designed to win votes, not to do what is best for the NHS44. This is a very serious credibility gap.