The nature of the crisis
The crisis in our care system
More people than ever before need our care system. The population is ageing and healthcare needs are longer lasting and more complex. These needs are not being met.
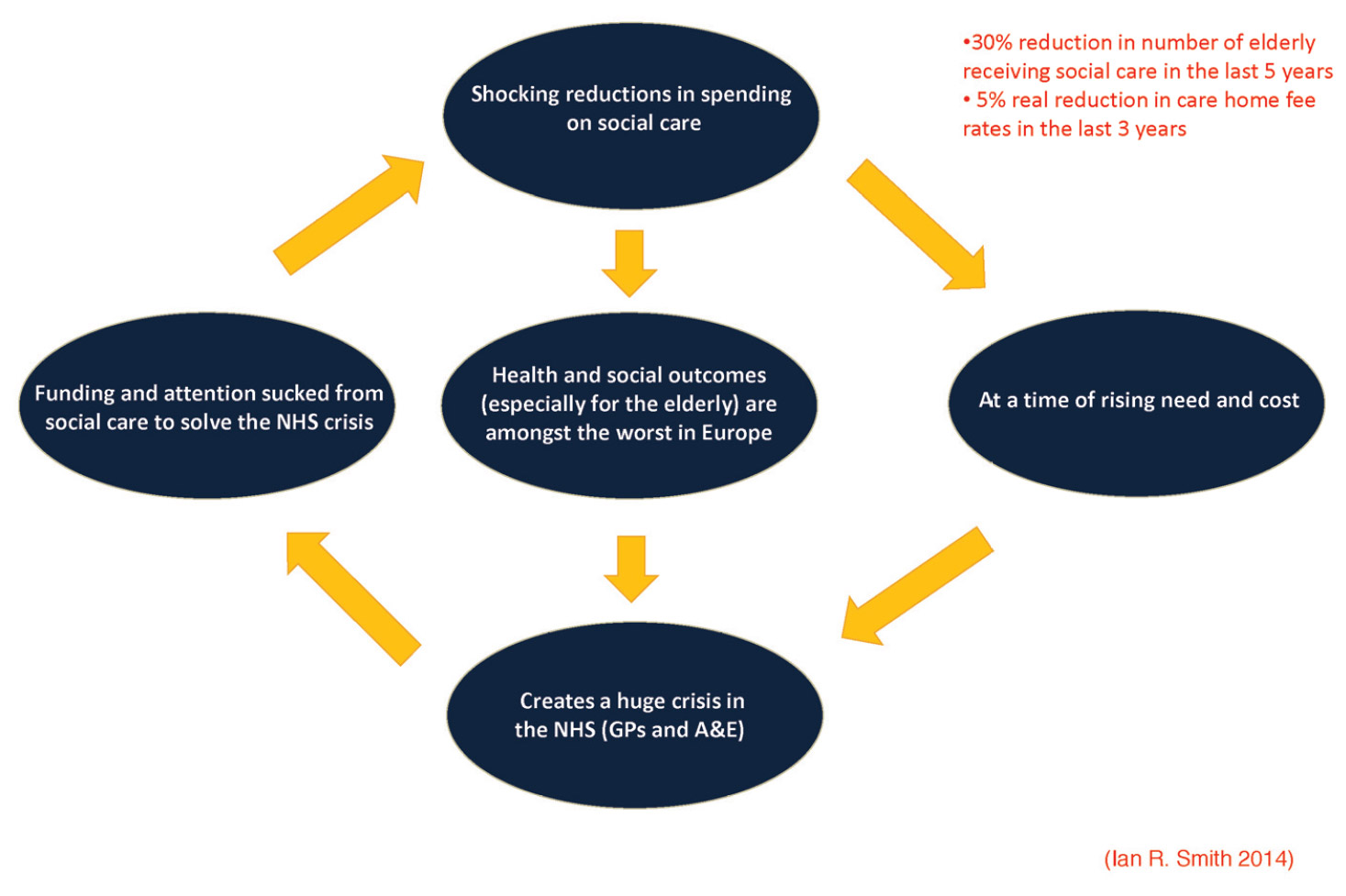
The introduction of austerity is such that there are more than 30 per cent fewer older people receiving social care now than five years ago2, rising to nearly 40 per cent when standardised for increased need3.
The precipitous fall in social care spending is occurring at a time when the population is getting older and co-morbidities and chronic diseases are increasing. These cuts represent a false economy. They result in increased spending in the NHS as more people – especially the most vulnerable like frail older people – inundate the health system.
Hospital “bed blocking” is very expensive, costing from £1,750 a week up to over £3,000 for an acute bed4 at end of life compared to about £800 to £1,000 for equivalent care in a nursing home bed5. Although worse in winter, it is a year-round issue. When he gave evidence to the House of Commons Health Select Committee in 2013, Mike Farrar – then chief executive of the NHS Confederation – suggested that an estimated 30 to 40 per cent of hospital beds are occupied by people who are there inappropriately6.
Moreover, inappropriate hospital stays for frail older people are dangerous and debilitating. The patient could receive the same or a better quality of nursing care in more appropriate surroundings, delivered by staff with specialist experience, and with less risk of hospital-acquired infections. This is not a sustainable or desirable state of affairs. It is expensive, and it is not producing the quality of care patients deserve.
The care system was a brilliant construct in 1948, but it is stuck in time
We do not have a system which is capable of giving us the care we need in the most appropriate setting. The main reason for this is that it is stuck in time.
The model of care was created in 1948 when the epidemiology of disease, social policy and people’s lives were very different from today. In that year, someone aged 65 would have had a life expectancy at birth of 44 years for men and 48 years for women.7 People died quite suddenly, most of the time within six months or less of contracting a disease.
The NHS was therefore founded on an acute care model, based on district general hospitals – which at the time performed relatively simple clinical procedures – and GP surgeries handling minor ailments. Social care was not a large part of the system.
The model has barely changed since. Our society has, however. For babies born between 2011 and 2013, life expectancy is 79 years for men and 83 years for women8. Today’s population ages slowly, living with chronic disease, and with co-morbidities. Men aged 65 today have a seven in 10 chance of needing some care before they die; women aged 65 nearly a nine in 10 chance9. An estimated two-thirds of those who have reached pensionable age have at least two chronic conditions10 and 850,000 people in the UK are living with dementia.11
The vicious circle of a broken down health and social care system
Mortality from non-communicable diseases (including cardiovascular and cancer) in 17 peer countries, 2008
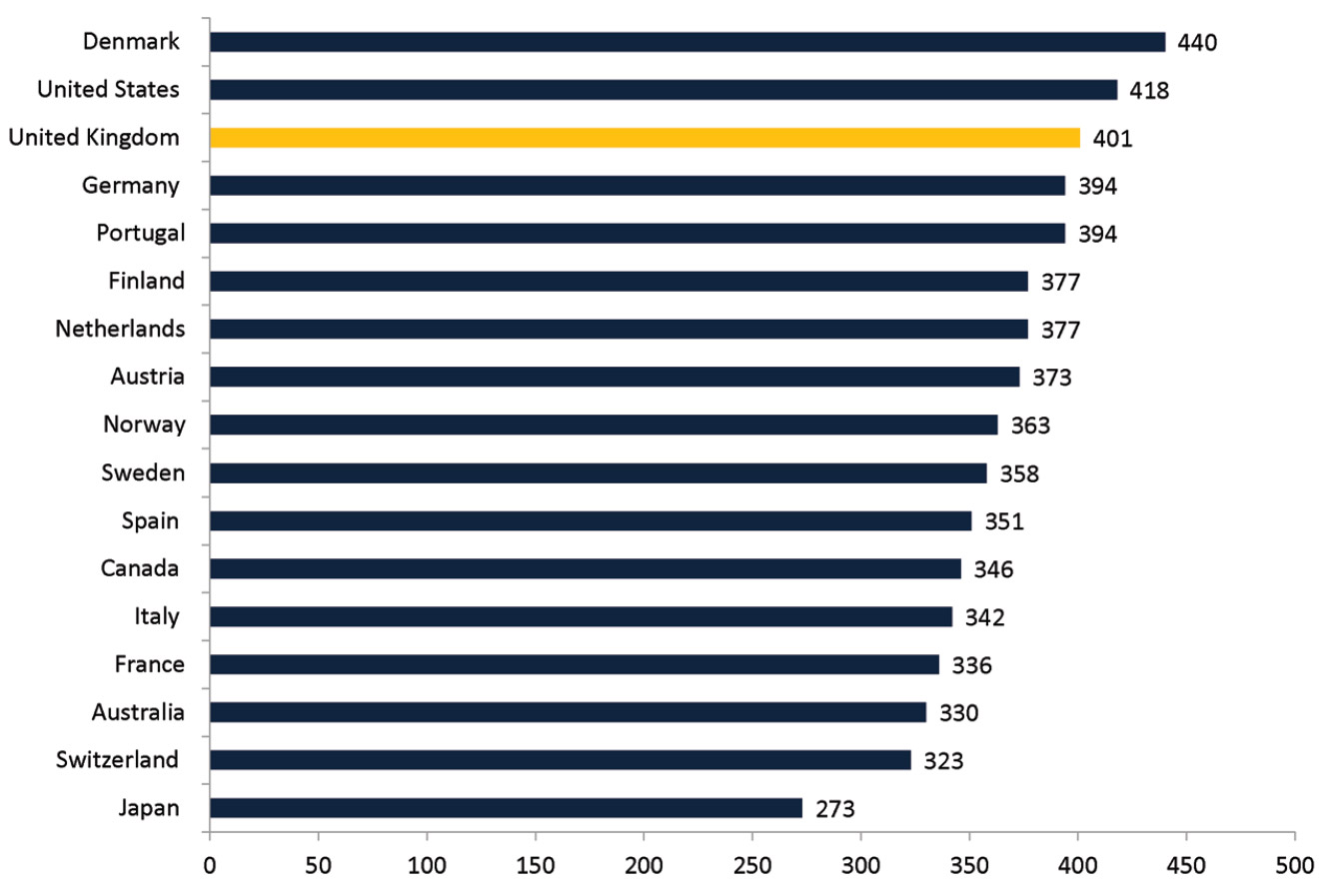
Organisation for Economic Co-operation and Development (OECD) data cited in Woolf, S. and Aron, L. (eds.) (2013) US Health in International Perspective: Shorter Lives, Poorer Health Washington, DC: The National Academies Press
These chronic diseases are often related to lifestyle issues. Obesity, for instance, represents a widespread threat to health and wellbeing in this country: a total of 61 per cent of adults are either overweight or obese.12 This is driving rises in conditions such as diabetes. In 2011/12 there were 2.6 million people aged over 17 diagnosed with diabetes in England13. By 2030, it is estimated that there will be more than four and a half million people aged 16 or over with the condition14.
This is a very different context from that of 1948, and we need a different care system as a result. Lower spending and higher need in social care, placing greater stress on the NHS, is a vicious spiral.
It is no coincidence that the United Kingdom has some of the worst health and social care outcomes in the developed world. For age-standardised deaths per 100,000 people for non-communicable diseases, the UK ranked 15 out of 1715.
What we need now
These demographic trends require a care system that offers a broad yet personalised service out of hospital, and consolidation of clinical units with scale in scientific discovery in hospital networks.